Dextrocardia
Cyanotic heart defect - dextrocardia; Congenital heart defect - dextrocardia; Birth defect - dextrocardia
Dextrocardia is a condition in which the heart is pointed toward the right side of the chest. Normally, the heart points to the left. The condition is present at birth (congenital).
Causes
During the early weeks of pregnancy, the baby's heart develops. Sometimes, it turns so that it points to the right side of the chest instead of the left side. The reasons for this are unclear.

There are several types of dextrocardia. Many types involve other defects of the heart and abdomen area.
In the simplest type of dextrocardia, the heart is a mirror image of the normal heart and there are no other problems. This condition is rare. When this occurs, the organs of the abdomen and the lungs will often also be arranged in a mirror image. For example, the liver will be on the left side instead of the right.
Some people with mirror-image dextrocardia have a problem with the fine hairs (cilia) that filter the air going into their nose and air passages. This condition is called Kartagener syndrome.
In the more common types of dextrocardia, other heart defects are also present. The most common of these include:
-
Double outlet right ventricle
(the aorta connects to the right ventricle instead of to the left ventricle)
Double outlet right ventricle
Double outlet right ventricle (DORV) is a heart disease that is present from birth (congenital). The aorta connects to the right ventricle (RV, the ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Endocardial cushion defect
(the walls separating all 4 chambers of the heart are poorly formed or absent)
Endocardial cushion defect
Endocardial cushion defect (ECD) is an abnormal heart condition. The walls separating all 4 chambers of the heart are poorly formed or absent. Also...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Pulmonary stenosis
(narrowing of the pulmonary valve) or
atresia
(pulmonary valve does not form properly)
Pulmonary stenosis
Pulmonary valve stenosis is a heart valve disorder that involves the pulmonary valve. This is the valve separating the right ventricle (one of the ch...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleAtresia
Pulmonary atresia is a form of heart disease in which the pulmonary valve does not form properly. It is present from birth (congenital heart disease...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Single ventricle (instead of two ventricles, there is a single ventricle)
-
Transposition of the great vessels
(the aorta and pulmonary artery are switched)
Transposition of the great vessels
Transposition of the great vessels is a heart defect that occurs from birth (congenital). The 2 major vessels that carry blood away from the heart -...
ImageRead Article Now Book Mark Article -
Ventricular septal defect
(hole in the wall that separates the right and left ventricles of the heart)
Ventricular septal defect
Ventricular septal defect is a hole in the wall that separates the right and left ventricles of the heart. Ventricular septal defect is one of the m...
ImageRead Article Now Book Mark Article
The abdominal and chest organs in babies with dextrocardia may be abnormal and may not work correctly. A very serious syndrome that appears with dextrocardia is called heterotaxy. In this condition, many of the organs are not in their usual places and may not work properly. For example, the spleen may be completely missing. The spleen is an important part of the immune system, so babies born without this organ are in danger of severe bacterial infections and death. In another form of heterotaxy, several small spleens exist, but they may not work correctly.
Heterotaxy may also include:
- Abnormal gallbladder system
- Problems with the lungs
- Problems with the structure or position of the intestines
- Severe heart defects
- Abnormalities of the blood vessels
Possible risk factors for dextrocardia include a family history of the condition.
Symptoms
There are no symptoms of dextrocardia if the heart is normal.
Conditions that may include dextrocardia may cause the following symptoms:
- Bluish skin
- Difficulty breathing
- Failure to grow and gain weight
- Fatigue
- Jaundice (yellow skin and eyes)
- Pale skin (pallor)
- Repeated sinus or lung infections
Exams and Tests
The health care provider will perform a physical exam and ask about the symptoms.
Tests to diagnose dextrocardia include:
- Chest x-ray
-
CT scan of the heart
CT scan of the heart
A computed tomography (CT) scan of the heart is an imaging method that uses x-rays to create detailed pictures of the heart and its blood vessels. Th...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Electrocardiogram
Electrocardiogram
An electrocardiogram (ECG) is a test that records the electrical activity of the heart.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
MRI of the heart
MRI of the heart
Heart magnetic resonance imaging is an imaging method that uses powerful magnets and radio waves to create pictures of the heart. It does not use ra...
ImageRead Article Now Book Mark Article -
Echocardiogram
Echocardiogram
An echocardiogram is a test that uses sound waves to create pictures of the heart. The picture and information it produces is more detailed than a s...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
A complete mirror image dextrocardia with no heart defects requires no treatment. It is important, however, to let the child's health care provider know the heart is on the right side of the chest. This information can be important in some exams and tests.
The type of treatment needed depends on the heart or physical problems the infant may have in addition to dextrocardia.
If heart defects are present with dextrocardia, the baby will most likely need surgery. Babies who are very ill may need to take medicines before they can have surgery. These medicines help the baby grow larger so surgery is easier to perform.
Medicines include:
- Water pills (diuretics)
- Drugs that help the heart muscle pump more forcefully (inotropic agents)
- Drugs that lower blood pressure and ease the workload on the heart (ACE inhibitors)
The baby might also need surgery to correct problems in the organs of the abdomen.
Children with Kartagener syndrome will need repeated treatment with antibiotics for sinus infections.
Children with a missing or abnormal spleen need long-term antibiotics.
All children with heart defects may need to take antibiotics before surgeries or dental treatments.
Outlook (Prognosis)
Babies with simple dextrocardia have a normal life expectancy and should have no problems related to the location of the heart.
When dextrocardia appears with other defects in the heart and elsewhere in the body, how well the baby does depends on the severity of the other problems.
Babies and children without a spleen may have frequent infections. This is at least partially preventable with daily antibiotics.
Possible Complications
Complications depend on whether dextrocardia is part of a larger syndrome, and whether other problems exist in the body. Complications include:
- Blocked intestines (due to a condition called intestinal malrotation)
- Heart failure
- Infection (heterotaxy with no spleen)
- Infertility in males (Kartagener syndrome)
- Repeated pneumonias
- Repeated sinus infections (Kartagener syndrome)
- Death
When to Contact a Medical Professional
Call your provider if your baby:
- Seems to get frequent infections
- Does not seem to gain weight
- Tires easily
Seek emergency care if your baby has:
- A bluish color to the skin
- Trouble breathing
- Yellow skin (jaundice)
Prevention
Some syndromes that include dextrocardia may run in families. If you have a family history of heterotaxy, talk to your provider before becoming pregnant.
There are no known ways to prevent dextrocardia. However, avoiding the use of illegal drugs (especially cocaine) before and during pregnancy may lower the risk of this problem.
Talk to your provider if you have diabetes. This condition may contribute to your risk of having a child with certain forms of dextrocardia.
References
Park MK. Chamber localization and cardiac malposition. In: Park MK, ed. Park's Pediatric Cardiology for Practitioners . 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:chap 17.
Webb GD, Smallhorn JF, Therrien J, Redington AN. Congenital heart disease. In: Mann DL, Zipes DP, Liby P, Bonow RO, Braunwald E, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine . 10th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 62.
-
Congenital heart defect overview
Animation
-
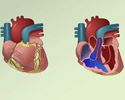
Dextrocardia - illustration
The heart is almost always located in the left side of the chest. Dextrocardia is a condition in which the apex of the heart is directed towards the right side of the chest. Dextrocardia can also cause the heart to develop in a mirror image of the normal heart. In the more common types of dextrocardia, heart defects are present in addition to the abnormal location of the heart.
Dextrocardia
illustration

-
Dextrocardia - illustration
The heart is almost always located in the left side of the chest. Dextrocardia is a condition in which the apex of the heart is directed towards the right side of the chest. Dextrocardia can also cause the heart to develop in a mirror image of the normal heart. In the more common types of dextrocardia, heart defects are present in addition to the abnormal location of the heart.
Dextrocardia
illustration
Review Date: 5/6/2016
Reviewed By: Scott I. Aydin, MD, Assistant Professor of Pediatrics, Albert Einstein College of Medicine, Division of Pediatric Cardiology and Critical Care Medicine, The Children's Hospital at Montefiore, Bronx, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Isla Ogilvie, PhD, and the A.D.A.M. Editorial team.